
Success stories can seem rare in the world of public health. And stories about the dentist in popular culture aren’t often the most enthusiastic.
But November’s SNAC Lab featured important dental success stories: Children’s oral health in Colorado is improving. At the same time, more Coloradans have dental insurance. These improvements have tracked with investments from local foundations, state spending, and changes in Medicaid’s oral health policies.
The SNAC Lab covered two new sets of data on oral health.
- Sara Schmitt, Director of Community Health Policy for the Colorado Health Institute (CHI), shared data about insurance coverage and dental care for adults and children from the 2017 Colorado Health Access Survey (CHAS).
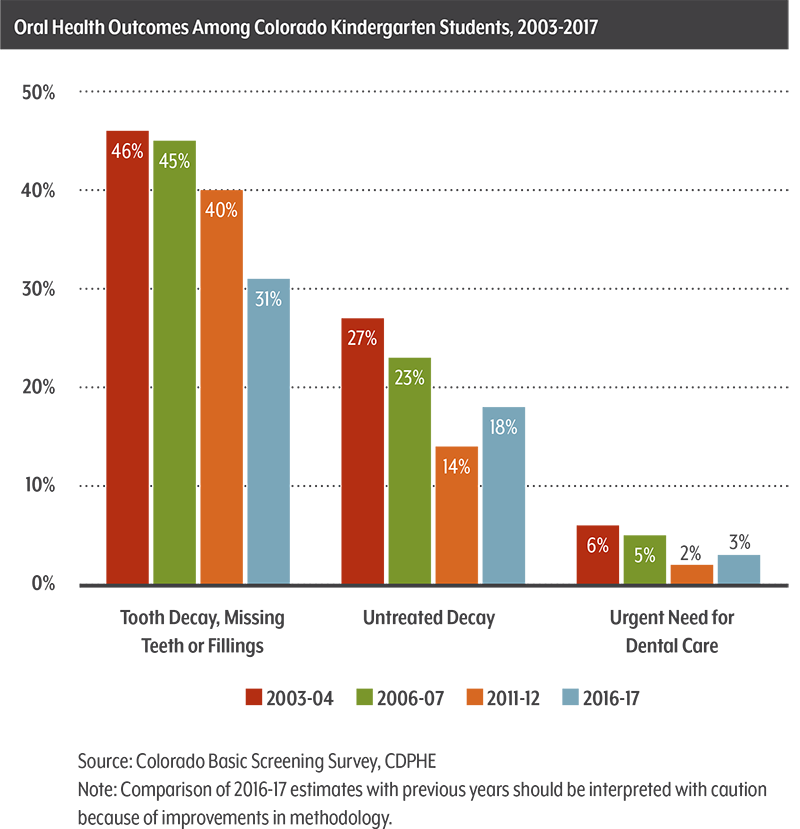
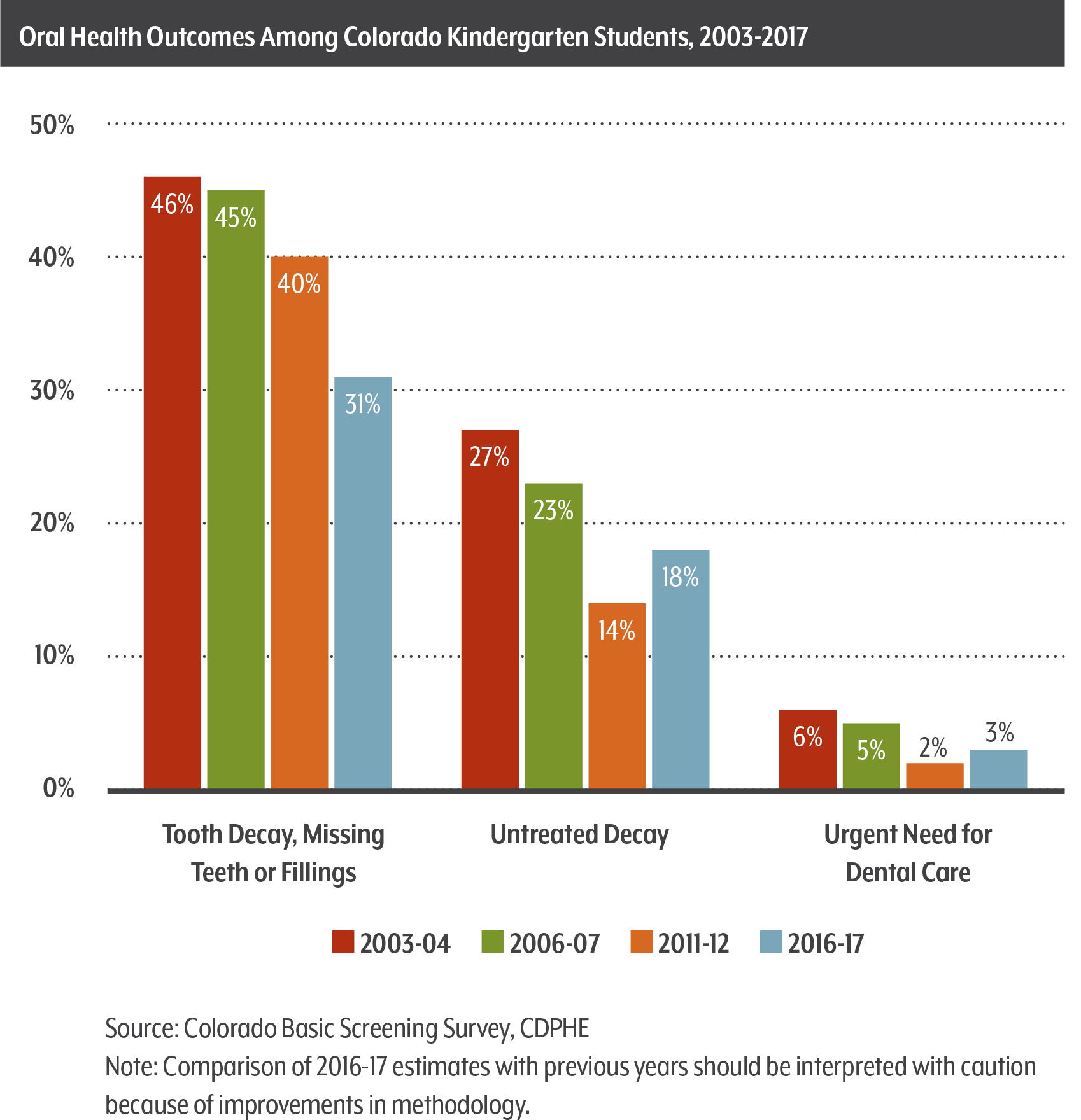
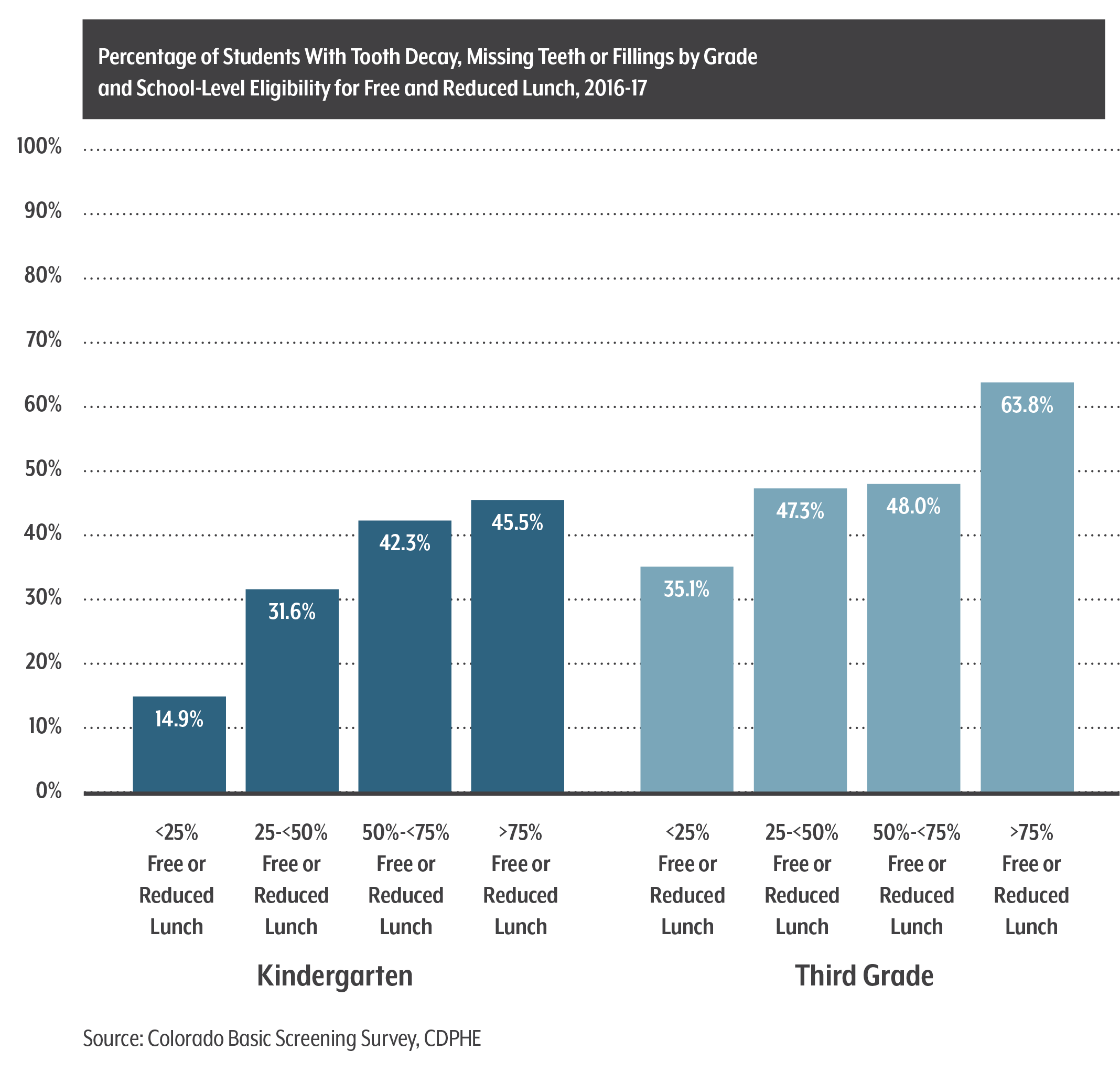
- Epidemiologist Renee Calanan and Dental Director Katya Mauritson, both of the Colorado Department of Public Health and Environment (CDPHE), shared the fiscal year 2016-17 results of Colorado’s Oral Health Basic Screening Survey.
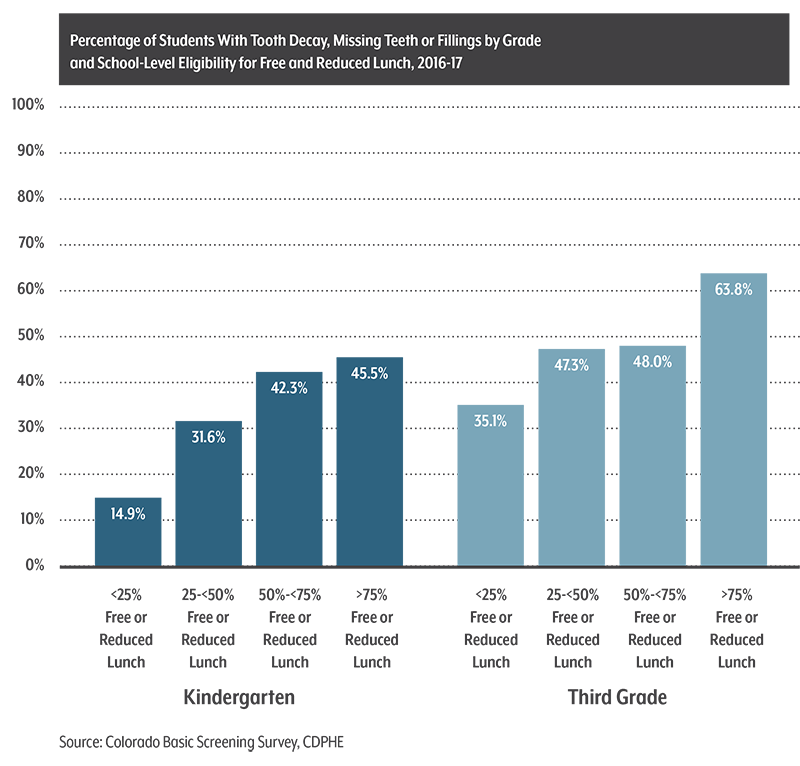
Healthier Teeth and More Coverage, But Disparities Remain
Physical and oral health are closely connected, Schmitt said. Nearly 90 percent of Coloradans in good physical health reported having good oral health on the 2017 CHAS while only half of those with poor physical health reported good oral health.
Seven of 10 Coloradans now have dental insurance (70 percent), up from 63 percent in 2009, according to the CHAS.
Low-income adults are less likely to have dental insurance than higher-income adults, though the rates for both have improved since 2013. Children are more likely to have dental insurance than adults: 85.3 percent of children are insured compared with 65.2 percent of adults.
But the percentage of Coloradans who actually visited the dentist held steady at around 66 percent.
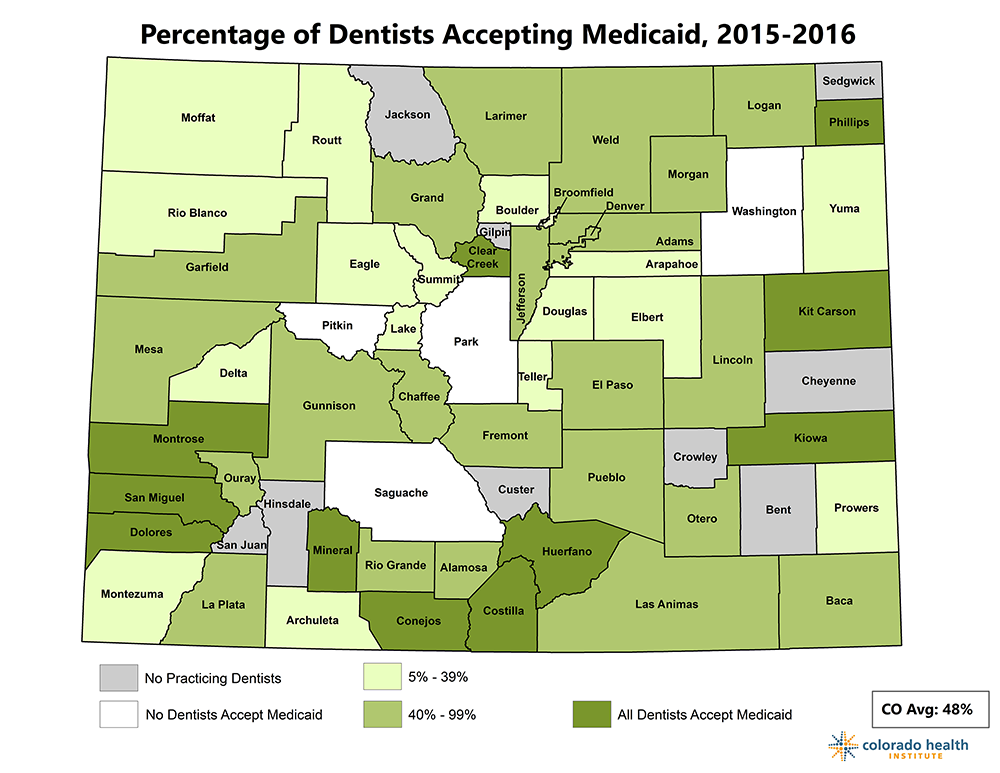
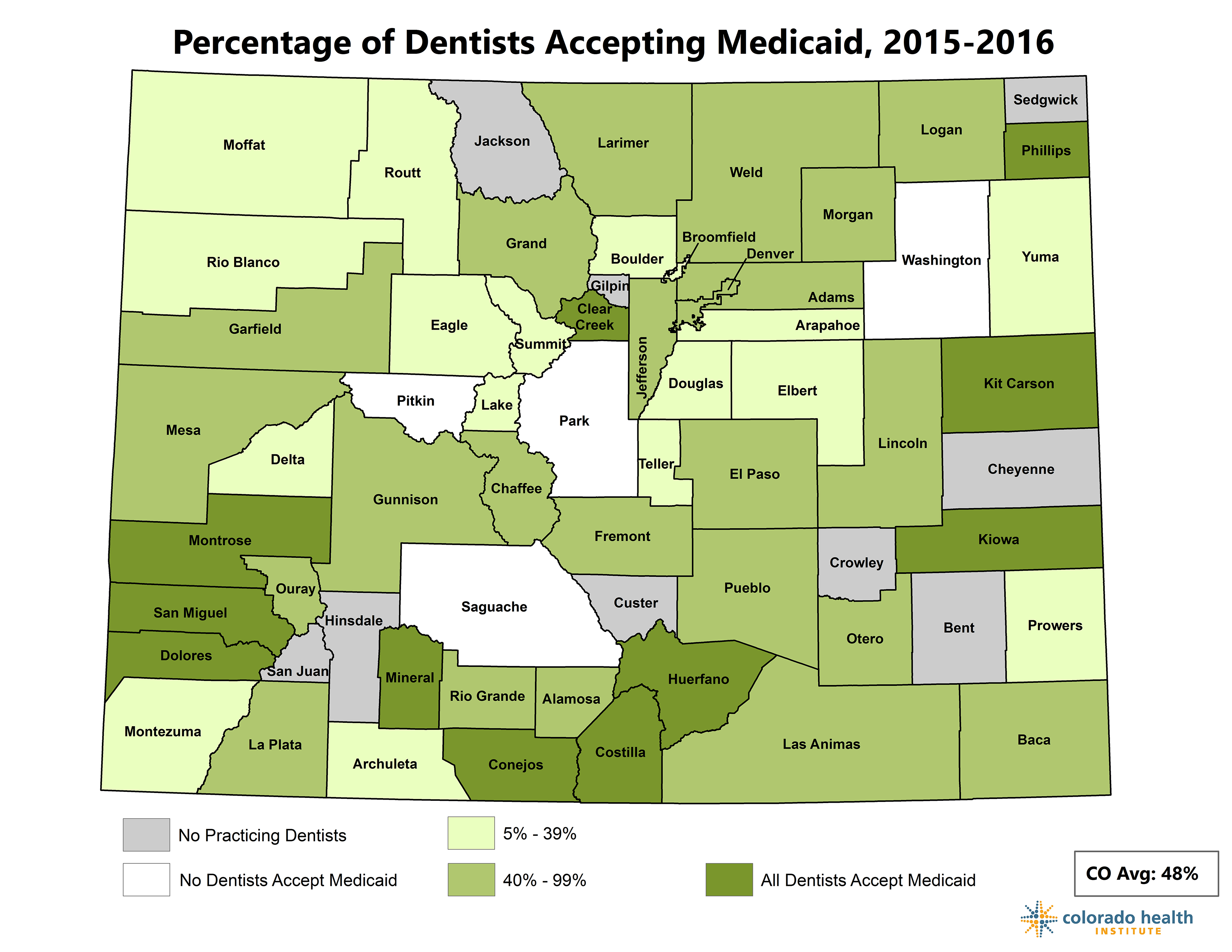
Unequal access to dental care may be to blame. Some counties don’t have dentists at all, and some have none that accept Medicaid, according to the CHAS. (See map.)
{kind=link}
{kind=link}
{kind=link}