Supporting Documents
Topics
Healthcare Costs
Health Coverage and the Uninsured
Legislation and Policy
The Cost Shift Myth
New State Report Suggests Existing Policies Haven’t Controlled Hospital Costs. Will New Strategies Be Needed?
February 13, 2019
March 10, 2023
Key Takeaways
Advocates for Medicaid expansion promoted the idea that hospitals charge extra to patients with private insurance to make up for underpayments from the uninsured and public programs.
A new report from Colorado’s Medicaid agency calls into question this theory of the “cost shift.”
Leading economists have debunked the cost shift, saying instead that hospital prices depend on market dynamics and competition.
Their reasoning was that if fewer patients were uninsured and Medicaid paid more, hospital prices — and insurance premiums — for privately insured patients would fall.
But a draft report1 released by Colorado’s Department of Health Care Policy and Financing (HCPF) in January backs up what health economists have been saying about the cost shift: It doesn’t exist.
The report shows that, contrary to expectations, Medicaid expansion did not lead to more affordable insurance premiums, and hospital prices continue to rise.
Addressing the Cost Shift
Two important policies have shaped Colorado’s health care landscape over the past decade. First, the legislature created the Hospital Provider Fee in 2009 to boost payments to hospitals to help them offset the cost of caring for people covered by Medicaid. Hospitals pay a fee, which attracts federal matching funds, most of which are paid back to hospitals along with the original fee. This creates a net positive for most hospitals.
Second, the ACA paved the way for Colorado to substantially expand Medicaid eligibility, covering more than 400,000 additional people (most of whom had previously been uninsured). As a result, hospitals received payments for many patients who could not pay before Medicaid expansion.
These two policies share a common goal: to use Medicaid payments to lessen the cost shift and thereby decrease the price of private insurance.
Controlling the High Cost of Private Insurance
Hospitals provide care to the uninsured but usually don’t get paid for those services. They can try to recoup these costs by charging other patients higher prices. This so-called cost shift is viewed by some as a hidden tax on people and businesses that buy insurance.
Policymakers have reasoned that expanded Medicaid coverage benefits everyone because less cost shifting could help control the rising price of private insurance.
For example, Gov. Bill Ritter, who signed the legislation that established the Hospital Provider Fee and began Medicaid expansion in Colorado, argued that it would “address cost-shifting and the high cost of uncompensated care, two of the main reasons for skyrocketing costs for small businesses and health care providers.”2
However, HCPF’s new report suggests that the Hospital Provider Fee and expansion of Medicaid have had little impact on the high price of insurance.
An Unfulfilled Hope
In theory, at least, the Hospital Provider Fee and the ACA could improve hospitals’ bottom lines and reduce the costs shifted to privately insured patients.
But in fact, these policies have done little to control the cost of private insurance.
Medicaid expansion and the accompanying drop in the uninsured population have reduced the amount of uncompensated care delivered in Colorado. Hospitals in Colorado lost roughly $700 million annually due to uncompensated care prior to Medicaid expansion. That amount dropped to about $300 million after expansion in 2014.1
Many of the uninsured gained coverage through Medicaid, and hospitals are now reimbursed for some of their costs.
However, hospitals and providers have long pointed out that government reimbursements through Medicaid and Medicare often don’t cover the actual cost of care, resulting in “undercompensated care.”
In 2009, Medicaid payments covered about 54 percent of the actual cost of care provided. But reimbursement increased to 69 percent of the cost of care by 2017, according to the HCPF report. Medicare payment rates have also increased slightly since 2009, but not enough to keep pace with the growth in hospital costs.
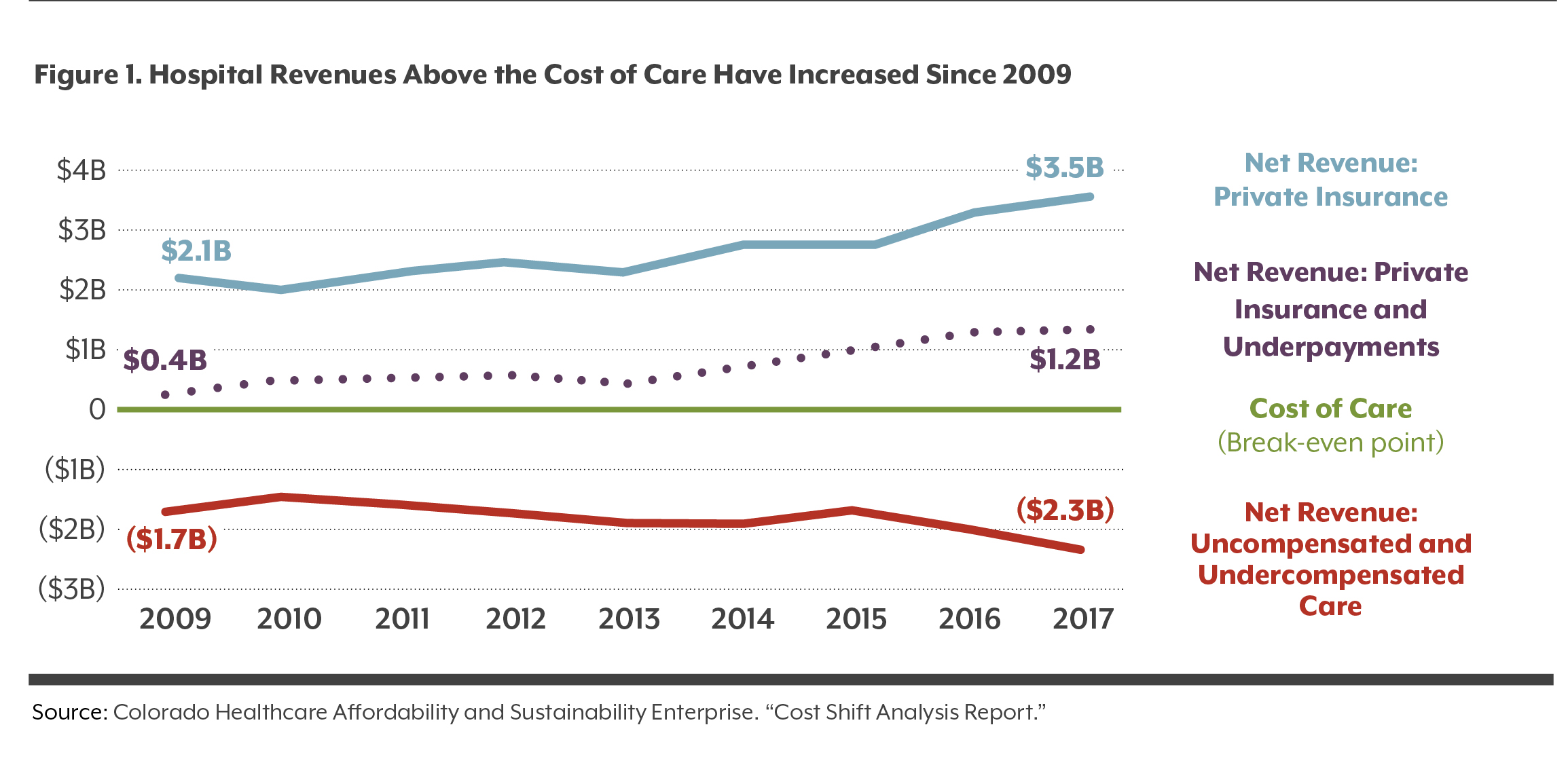
In total, uncompensated and undercompensated care in Colorado amounted to $2.3 billion in 2017 (see Figure 1). This shortfall is the amount by which the cost of care exceeded reimbursements. The shortfall has increased by about 34 percent since 2009, when there was a $1.7 billion difference between the cost of care and reimbursements.
Those shortfalls are more than offset by private insurance payments to hospitals. Private insurance paid hospitals $3.5 billion more than it cost to provide care in 2017. That is $1.2 billion more than what would be needed to exactly offset the $2.3 billion shortfall in 2017. The HCPF report questions whether this “overcompensation” is justified. As shown in Figure 1, the amount of compensation over the break-even point has grown substantially since 2009, when it stood at $400 million.
HCPF’s estimate of overcompensation will be controversial because it implies that hospitals should break even on the services they offer and not make a profit or put away cash reserves. There could be many explanations for why the surplus varies over time, including changing patient demographics and health care needs. In addition, HCPF’s analysis is based on aggregate hospital data that could obscure important differences across hospitals and geographic regions.
The HCPF report argues that policymakers need to further scrutinize the causes of this apparent surplus and what hospitals are using it for. For example, HCPF suggests that hospitals are overbuilding new hospital facilities on the Front Range and using revenues from private insurers to foot the bill. However, HCPF’s report also notes that the number of hospital beds per capita in Colorado is well below the national average.
The Cost Shift Myth
Evidence shows that the policies intended to address hospital cost shifting have not been effective at reining in the costs borne by private insurance. If anything, the situation has worsened.
This should not be a surprise. Although the cost shift theory sounds logical, most economists have found that what hospitals charge private insurance actually has little to do with how much money they may be losing on Medicare, Medicaid, or the uninsured.3
Studies have found that the prices paid by private insurance depend primarily on competitive market dynamics among hospitals and insurance companies. If hospitals have market power when they negotiate prices with a private insurer, they can use that leverage to charge higher prices, regardless of the amount of undercompensated care they have.
Hospitals’ market power may be increasing in Colorado, according to the HCPF report. In 2009, six hospital systems controlled 23 hospitals, but by 2017, seven systems controlled 41 hospitals. Some hospitals are also increasing their market power by acquiring physician groups, which can allow them to influence where patients are sent for hospital care.
Recent studies reveal that changes in government payment rates have little or no effect on private insurance. In fact, some studies show that hospitals dealing with cuts in government payment rates have lowered private insurance payments — the opposite of what the cost shift theory predicts.
How could this be? Hospitals can respond to lower government payments by reducing their operating costs and charging all patients less — those with private insurance or government coverage. Or hospitals may respond by reducing prices for private insurers in order to attract more patients with high-paying private coverage.
Conclusion
The HCPF report is an attempt to frame a billion-dollar debate over the role of hospitals in Colorado.
State leaders once promoted the theory of the cost shift as a rationale to create the Hospital Provider Fee and expand Medicaid. The HCPF report builds a convincing case that paying hospitals more for Medicaid and uninsured patients does not lower costs for people with private coverage.
As a result, policymakers will need to consider new ideas to actually bring down charges for everyone.
One option involves the Hospital Provider Fee, which has been a windfall for hospitals. In FY 2017-18, hospitals paid nearly $900 million in fees into the program but received $1.3 billion — a net gain of $400 million for Colorado hospitals.
HCPF wants to redesign the provider fee to use some or all of that $400 million to incentivize hospitals to find ways to charge less and provide better care that is more integrated with their communities. The effort is known as the Hospital Transformation Program.
This is one of several policy proposals at the state Capitol to cut health care costs. CHI is tracking these ideas closely. See www.coloradohealthinstitute.org/analysis for our recent work.
Endnotes
1 Colorado Healthcare Affordability and Sustainability Enterprise. “Cost Shift Analysis Report.” Draft, January 22, 2019. Available at: https://www.colorado.gov/pacific/sites/default/files/2019%20January%20HCPF%20Cost%20Shift%20Analysis%20Report%20Draft.pdf
2 Office of the Governor. “2007-2009 Ritter Administration Accomplishments.” Available at: http://hermes.cde.state.co.us/drupal/islandora/object/co%3A7731/datastream/OBJ/download/2007-2009_Ritter_administration_accomplishments.pdf
3 See for example: Frakt AB, “How Much Do Hospitals Cost Shift? A Review of the Evidence,” The Milbank Quarterly, 2011;89(1):90-130. White C, “Contrary to Cost-Shift Theory, Lower Medicare Hospital Payment Rates for Inpatient Care Lead to Lower Private Payment Rates,” Health Affairs, 2013;32(5):935-943. Wu VY, “Hospital Cost Shifting Revisited: New Evidence from the Balanced Budget Act of 1997,” International Journal of Health Care Finance and Economics, 2010;10(1):61-83.