Colorado Access to Care Index Data Sources and Methods
The Colorado Access to Care Index is based on five data sources outlined below.
Colorado Health Access Survey (CHAS)
What It Is: The Colorado Health Access Survey – the CHAS – is the premier source of information on health insurance coverage, access to health care, and how health care is used in Colorado. More than 10,000 randomly selected households participated in the 20-minute survey. The data are statistically weighted to be representative of the state’s population. The CHAS is fielded, analyzed and managed by the Colorado Health Institute. It is funded by The Colorado Trust.
Time Points: Data are available from 2009, 2011, 2013 and 2015.
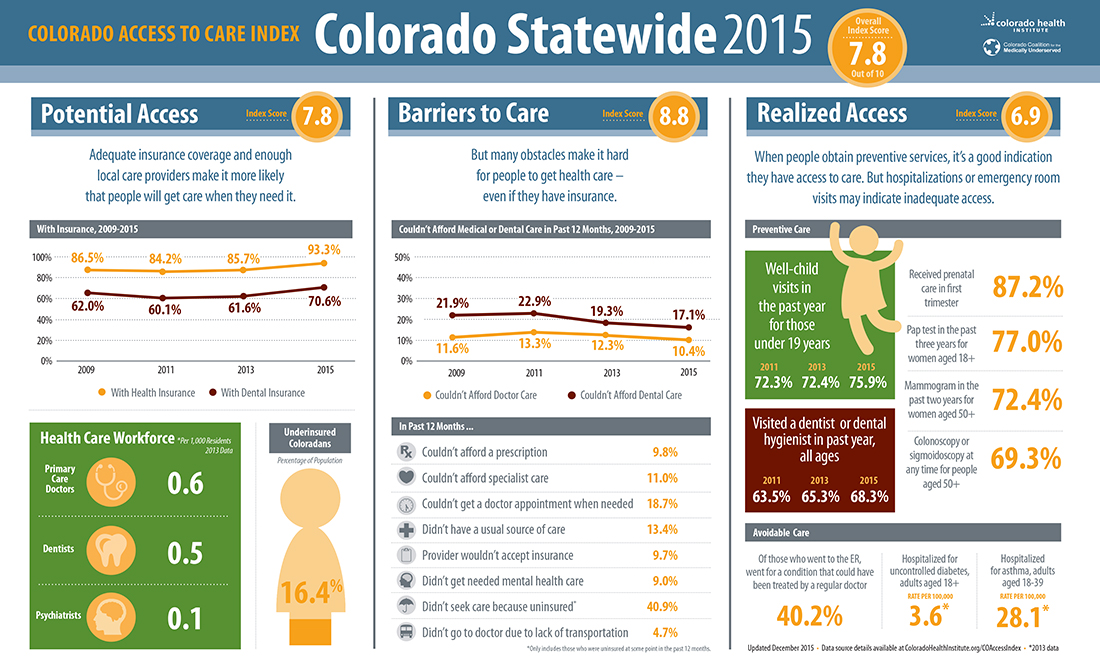
CHAS Metrics Used: Potential Access
- Coloradans with or without health insurance at the time of the survey.
- Coloradans who are adequately insured or underinsured for medical care in the past 12 months.
- The CHAS defines underinsurance for families earning at least 200 percent of the federal poverty level (FPL) as spending as least 10 percent of annual income on out-of-pocket medical expenses, not including the cost of purchasing health insurance. For families below 200 percent FPL, underinsurance is defined as spending at least five percent of annual income on out-of-pocket medical expenses.
- The CHAS defines adequately insured as those who had coverage for all of the 12 months prior to the survey, did not meet either of the two out-of-pocket cost definitions of underinsurance, and did not have an uninsured family member.
- Coloradans with or without dental insurance at the time of the survey.
Barriers to Care
- No usual source of care (other than the emergency department).
In the past 12 months
- Did not see a doctor due to cost.
- Did not fill a prescription due to cost.
- Did not see a specialist due to cost.
- Did not get dental care due to cost.
- Unable to get an appointment at the doctor’s office as soon as you thought one was needed.*
- Unable to find transportation to the doctor’s office or the doctor’s office was too far away.
- Told by the doctor’s office they weren’t accepting patients with your type of health insurance.
- Needed mental health care or counseling but didn’t get it at that time.*
- Did not seek an appointment because you were uninsured.*
* Asked for the first time in 2013.
Realized Access
- Visited a dentist or dental hygienist in the past 12 months.
- Well-child visits (visit for a check-up, physical examination or other preventive care) for those under age 19 in the past 12 months.
- Of those who visited a hospital emergency room in the past 12 months, those who went for a condition that could have been treated by a regular doctor if one had been available.
Notes and Limitations:
- The Colorado Health Access Survey is conducted every other year. The complete survey form is available here.
- The “did not seek an appointment because you were uninsured” indicator should be interpreted with caution. Because the denominator – the number of uninsured Coloradans – has become smaller for this variable across the 21 health statistics regions (HSRs) after the implementation of the Affordable Care Act (ACA), some of these estimates have large margins of error.
MedicalQuest
What It Is: A database of practicing providers across Colorado.
Time Points: MedicalQuest data from 2013 were used for the Colorado Access to Care Index.
MedicalQuest Metrics Used:
Potential Access
- Primary care physicians.
- Nurse practitioners.
- Physician assistants.
- Dentists.
- Psychiatrists.
Notes and Limitations: MedicalQuest provides an estimate of practicing providers. The Colorado Health Institute calculated rate of providers per 1,000 residents using MedicalQuest data on the number of providers in each county and county population estimates from the Colorado Demography Office. Due to changes in MedicalQuest data collection methodology, 2015 data were not available at the time of the 2015 index update. Because we did not anticipate major changes in the workforce between 2013 and 2015, we felt it was reasonable to hold these data points constant at 2013 values for the 2015 update.
Colorado Pregnancy Risk Assessment Monitoring System (PRAMS)
What It Is: Annual survey funded by the Centers for Disease Control and Prevention (CDC) and administered by the Colorado Department of Public Health and Environment (CDPHE). The PRAMS is designed to monitor the experiences of Colorado women before, during and after pregnancy. The survey is mailed to a sample of women who have recently given birth. The survey data are weighted to be representative of Colorado’s population of women who recently gave birth.
Time Points: Annual survey. The Colorado Access to Care Index used 2009, 2010 and 2011 data for the first index because these were the most recent PRAMS data available as of March 2015. The updated Colorado Access to Care Index uses data from 2011, 2012 and 2013.
PRAMS Metric Used:
Realized Access
- Received prenatal care in first trimester of pregnancy was used in the updated version of the Colorado Access to Care Index, released in October 2015.
Notes and Limitations: Due to the small sample size of the PRAMS, we averaged three years of data to calculate stable estimates. The question asking mothers about whether they received prenatal care as soon as they wanted — used in the first version of the index — was dropped from the PRAMS survey. The updated version of the Colorado Access to Care Index included data on women who received prenatal care in the first trimester of pregnancy. Data from 2009-2011 show that at the state level the percentage of women receiving prenatal care as soon as they wanted was very similar to the percentage of women receiving prenatal care in the first trimester.
Colorado Behavioral Risk Factor Surveillance System (BRFSS)
What It Is: The BRFSS is an annual survey of Coloradans ages 18 years and older funded by the CDC and administered by CDPHE. The survey includes questions on lifestyle and behaviors related to leading causes of death and disease. Topics include smoking, overweight/ obesity, physical activity and use of preventive health services. The data are weighted to be representative of Colorado’s adult population.
Time Points: The BRFSS is conducted annually, though cancer screening questions are only asked in even numbered years. Therefore, we included the most recent BRFSS data available from 2012 in the first calculation of the index, released in March 2015, and 2014 BRFSS data in the updated index, released in October 2015.
BRFSS Metrics Used:
Realized Access
- Pap test in the past three years for women age 18 years and older.
- Mammogram in the past two years for women age 50 and older.
- Colonoscopy or sigmoidoscopy at any time for people age 50 and older.
Notes and Limitations:
- The 2012 BRFSS data are displayed in the Colorado Access to Care Index tables under 2013. The 2014 BRFSS data are displayed under 2015.
- Because of changes in survey methodology, data collected in 2012 or after cannot be compared to previous years.
Hospital Admissions Data
What It Is: The Colorado Hospital Association (CHA) compiles admissions data received from all Colorado acute care hospitals. The Colorado Health Institute included two metrics of potentially preventable hospitalizations — uncontrolled diabetes and asthma — in the Colorado Access to Care Index. These metrics quantify hospitalizations that might have been prevented if the patient had access to adequate primary care services in the community. Working with the Colorado Health Institute, CHA calculated the rate of preventable hospitalizations — also called Prevention Quality Indicators — using software developed by the Agency for Healthcare Research and Quality (AHRQ).
Time Points: CHA collects admissions data monthly. The Colorado Access to Care Index uses 2013 data, the most recent full year available. More recent data were not available when the Colorado Access to Care Index scores were updated in October 2015, so these values were held constant using 2013 data.
Metrics Used:
Realized Access
Hospital Admissions Data:
- Uncontrolled diabetes, adults age 18 and older.
- Asthma, young adults age 18 to 39.
Notes and Limitations:
- CHA provided these data at the county level. The Colorado Health Institute calculated estimates for each health statistics region (HSR) that include more than one county. We accomplished this by summing the number of cases in those counties then dividing by U.S. Census Bureau population estimates provided by AHRQ. The data are presented as rates per 100,000 population.
- These rates do not account for regional variation in health status. CHA’s risk-adjusted data could not be aggregated at the regional (HSR) level. Alternately, the Colorado Health Institute used the observed (unadjusted) data on hospital admissions.
Selection of Metrics
The following criteria were used to select the metrics included in the Colorado Access to Care Index:
- Validity: Metrics of factors known to increase potential access to care, barriers to care identified by consumers, and services used that suggest adequate access or insufficient access to primary care.
- Geography: Data that are available at the sub-state level. This allows the index to show differences between communities.
- Subgroups: Metrics that demonstrate access to care for Coloradans with all kinds of insurance, in regions across the state, belonging to different racial and ethnic groups and at different income levels. Some metrics are only available for, or only applicable to, particular age groups.
- Available over time: Metrics that allow the index to be updated and show changes over time. Most data sources included are expected to be available in the future, although not all are available retrospectively.
Calculating Index Scores
The scoring methodology was modeled after the National Health Security Preparedness Index, a collaborative effort of the Association of State and Territorial Health Officials, the Robert Wood Johnson Foundation and others.
The Colorado Health Institute first compiled the data for each of the metrics within the Potential Access, Barriers to Care and Realized Access sections. We used the most recent data available to calculate the index score.
The Colorado Access to Care Index score released in March 2015 mostly used 2013 data, with a few exception described above. The 2013 data provide a baseline measure of access to care in Colorado before major ACA policy changes — such as expanded Medicaid eligibility — when into effect in 2014.
The updated index provides a picture of “post-ACA” access to care in Colorado. This mostly used data from 2015, with a few exceptions described above.
Establishing Benchmarks
The first step in calculating the index was to establish an aspirational benchmark. In other words, we established a goal of either zero or 100 percent for most of the metrics. For example, we proposed an aspirational goal of 100 percent of Coloradans covered by health insurance. Alternately, we would aspire to the goal that no one in Colorado — zero percent — would experience a barrier such as not getting needed mental health care or not being able to afford a specialist.
For the metrics that are expressed as rates — such as for workforce and preventable hospitalizations — we based the goals on established benchmarks in the research literature and CHI’s past analyses. We used the best performing region as the aspirational goal when we were unable to identify a benchmark.
Calculating the Scores
Next, we converted each of the data metrics to a score on a scale of zero to one, where zero represents no access to care and one represents universal access. For example, 84.2 percent became .842.
This step required a few of the metrics — such as those in the Barriers to Care section — be mathematically “flipped” so that zero indicates a poor score and a score of one is “good.”
For example, 11.2 percent of Coloradans couldn’t afford a prescription in 2013. We converted the percentage to a score (.112) and then subtracted it from one (1- .112 = .888). We then averaged the scores across all the metrics within each of the three components — Potential Access, Barriers to Care and Realized Access. The average was then multiplied by 10. This step resulted in an overall score for Potential Access, an overall score for Barriers to Care and an overall score for Realized Access. Finally, we averaged the three component scores to calculate the overall score.