

Colorado’s Medicaid program — called Health First Colorado — is poised to take another step along the trail it blazed six years ago.
The state is preparing to implement the next phase of its Accountable Care Collaborative (ACC), a groundbreaking effort aimed at changing how care is delivered to Medicaid members as well as stemming the spending growth that saw Medicaid take up a bigger share of the state budget.
The ACC has huge implications for Colorado. More than one of five Coloradans is enrolled in Medicaid. And most of those members are in the ACC.
Phase One of the ACC has shown promise — modest cost savings as well as incremental increases in the use of services that can improve health. Phase Two, which is slated for 2018, outlines a broader range of policy changes and payment carrots and sticks that attempt to accelerate improvements in care and result in greater cost savings.
It is designed to influence, through contractually defined incentives and deterrents, the behaviors of the regional management entities created during Phase One as well as participating health care providers and Medicaid members themselves.
So, what does Phase Two mean for Colorado? The Colorado Health Institute (CHI) identified five primary themes for Phase Two related to the policy and payment changes:
- Paying for Care: A Few Sticks, Many Carrots. The way Medicaid pays health care providers remains largely unchanged. However, Phase Two — using contracts with regional entities —encourages greater quality and efficiency through approaches that reward better performance.
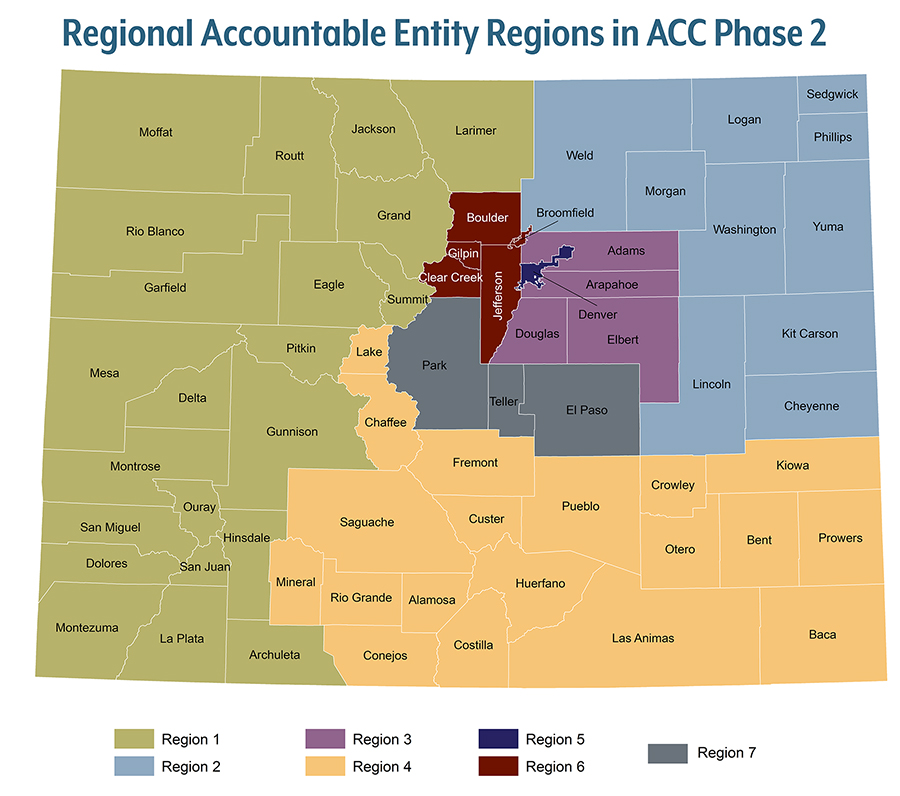
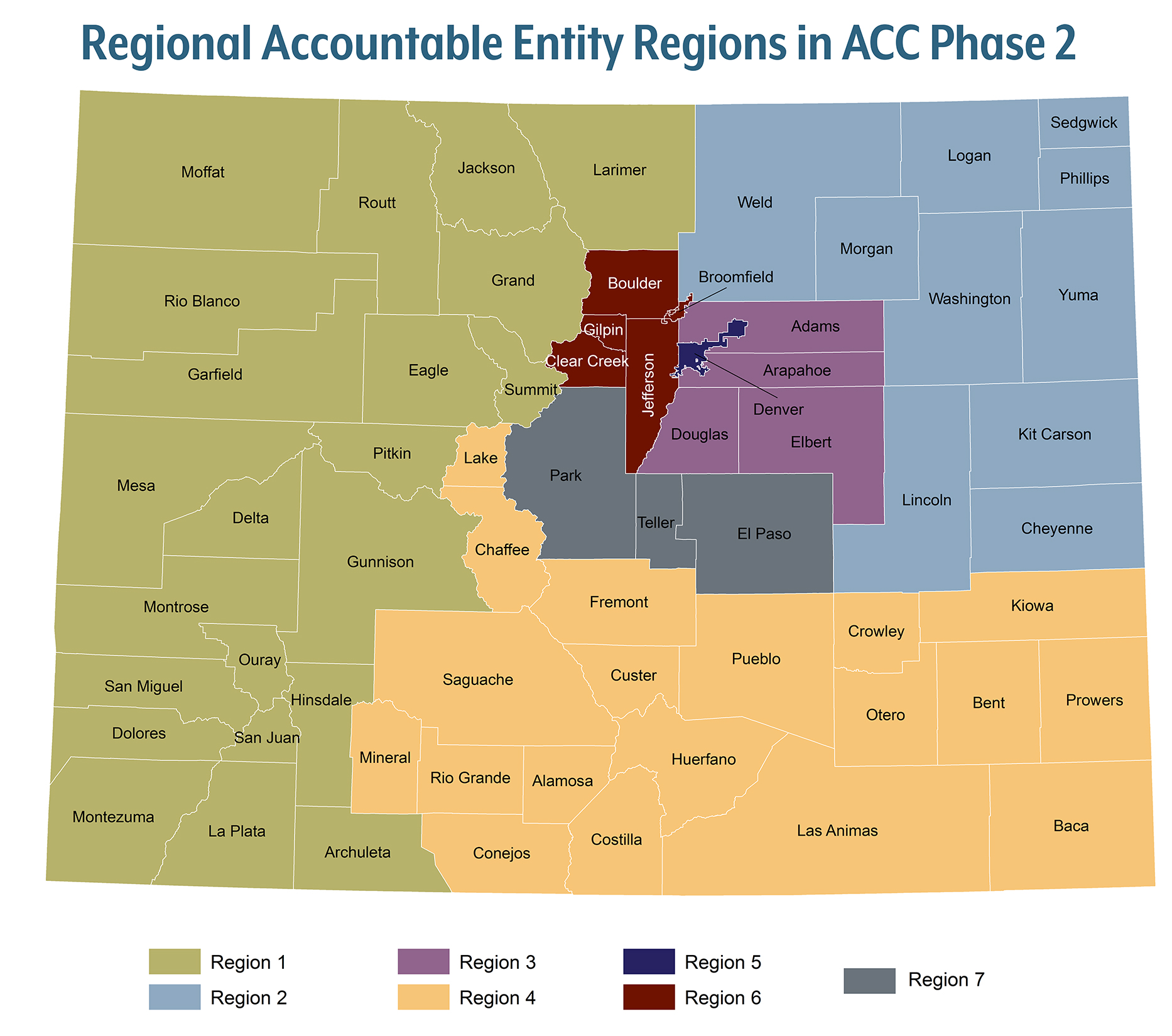
- Integration Moves Ahead. Phase Two will replace Regional Care Collaborative Organizations (RCCOs) and Behavioral Health Organizations (BHOs) with Regional Accountable Entities, or RAEs, in 2018. RAEs will connect Medicaid members with primary and behavioral health care.
- Welcome to the (Health) Neighborhood. Phase Two takes small steps in acknowledging factors beyond clinical care that influence health, such as education and housing.
- Access to Care is Location, Location, Location — and Past Use. Phase Two pays more attention to geography, with additional guidelines designed to improve access to care for rural Medicaid members. Medicaid members will be connected to primary care based on where they’ve sought care in the past rather than where they live.
- Doing It Up with Data. New data systems and required performance metrics attempt to support RAEs and providers in new ways, with the goal of improving care efficiency.
The steps outlined for Phase Two signal some big changes for the state’s primary care and behavioral health care providers. At the same time, Phase Two represents the next step along the trail toward greater substantive change.
{kind=link}