School-based health care becomes important part of rural safety net
Colorado’s rural residents face unique challenges when it comes to health care. Their insurance premiums are among the highest in the state, getting to a doctor may require a long ride, and providers such as dentists and physicians can be hard to come by.
School-based health centers (SBHCs) offer one response to these challenges.
Colorado now has 58 SBHCs. Forty-one of the 58 SBHCs that responded to a 2015-16 survey are urban, concentrated along the Front Range.
Colorado’s rural SBHCs, meanwhile, have increased from three to 17 in the decade since the Colorado Health Institute (CHI) and the Colorado Association for School-Based Health Care (CASBHC) conducted the first SBHC survey in the 2006-07 school year. SBHCs serve more than 36,000 users, up from 20,964 10 years earlier, according to the latest survey. Most users are students, though some SBHCs also serve siblings of students or the entire pediatric population in the county (ages 0-21).
SBHCs, located on school grounds or within a school, are operated by health care organizations that employ a medical provider, such as a nurse practitioner or physician assistant, to provide primary care. Most SBHCs also offer behavioral and oral health care on site.
In rural Colorado, especially, SBHCs fill gaps in health care. For example, oral health services, including cleanings, fluoride varnish application and sealants, are offered at a higher percentage of rural SBHCs than SBHCs in urban areas, where dental services are more prevalent.
There are other differences between rural and urban sites, the 2015-16 survey shows. Among them:
State funding makes up the largest portion (58 percent) of annual revenue for rural SBHCs. In urban SBHCs, patient-related revenue, such as Medicaid reimbursements, is the primary source of funding.
Most urban users are covered by Medicaid. Rural SBHCs see a higher percentage of privately insured and uninsured users than urban SBHCs.
While rural locations offer more dental services, urban SBHCs provide more birth control options.
The new survey results inform answers to these questions:
How does funding differ between urban and rural SBHCs in Colorado?
How do users differ between urban and rural school-based health centers?
How do services differ between urban and rural school-based health centers?
Answers show the important role that rural SBHCs continue to play in filling the provider gap.
Revenue
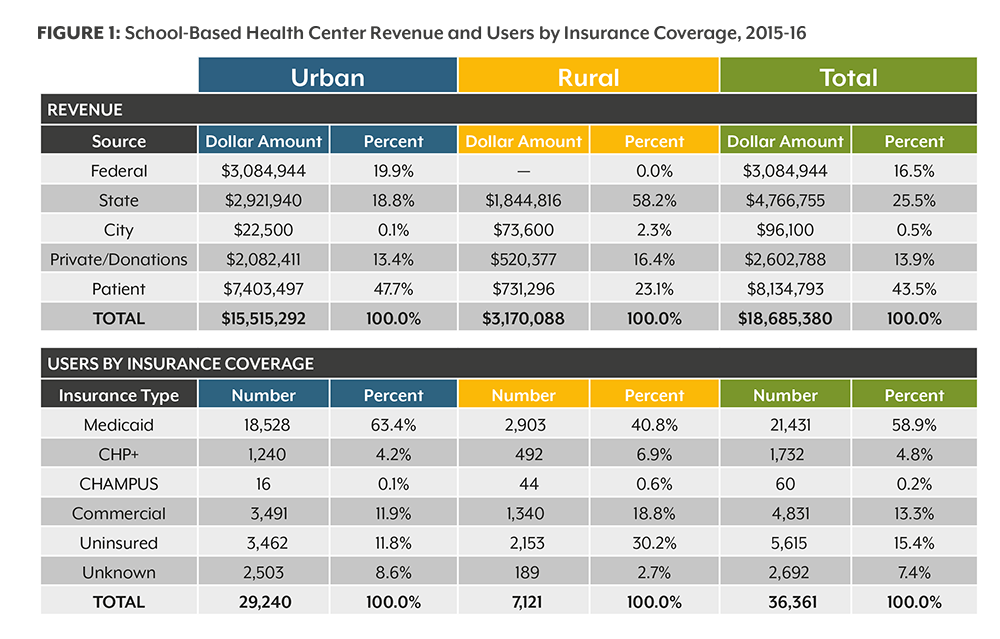
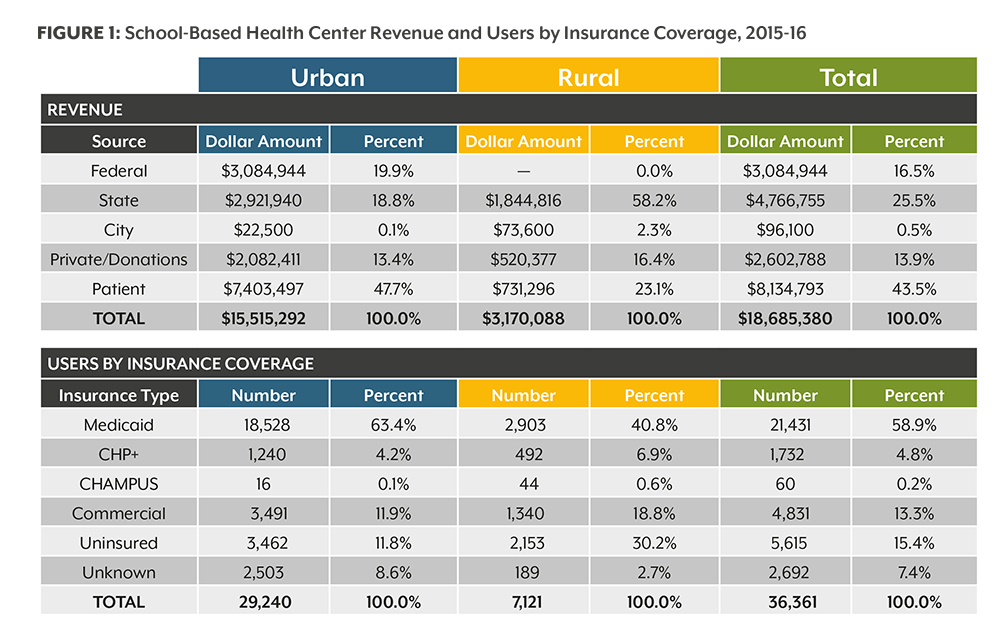
The legislature’s most recent allocation for SBHCs —$5 million for fiscal year (FY) 2017-18 — is managed by he Colorado Department of Public Health and Environment (CDPHE). Eleven SBHCs did not receive funding from CDPHE in the 2015-16 school year. These sites are in both urban and rural areas of the state. State funding accounts for more than half (58 percent) of total revenue for rural SBHCs compared with nearly 19 percent for urban SBHCs. Nearly half of the income of urban SBHCs (48 percent) comes from users; for rural SBHCs, it’s 23 percent (See Figure 1 below).
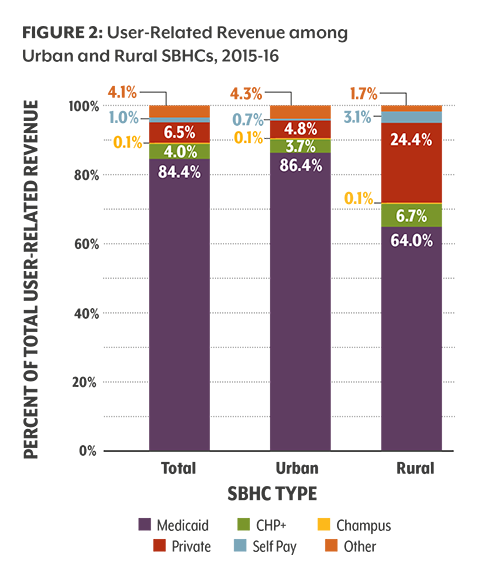
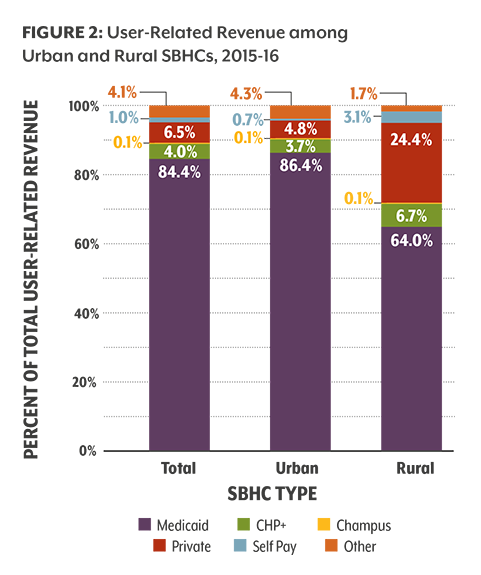
Medicaid contributes more than 80 percent of patient-related revenue in urban SBHCs compared with a little more than 60 percent among rural SBHCs. Rural SBHCs receive almost a quarter of their income from private insurance; for urban SBHCs, it’s 4.8 percent (See Figure 2). Rural users with private coverage may see SBHCs as more convenient and a better value in some circumstances.
Federal funds make up almost 20 percent of urban revenue in the 2015-2016 school year. For the same time period, rural SBHCs did not report receiving any federal funds (See Figure 1). It is important to note that rural SBHCs operated by federally qualified health centers (FQHC) receive at least indirect federal support based on the FQHC designation.
SBHC Users
In the 2015-16 school year, more than 36,000 users received care at Colorado’s SBHCs (see Figure 1). This record-setting number reflects the growth of this important model in the past 10 years.
In both rural and urban areas, SBHCs serve a disproportionate percentage of uninsured and Medicaid enrollees.
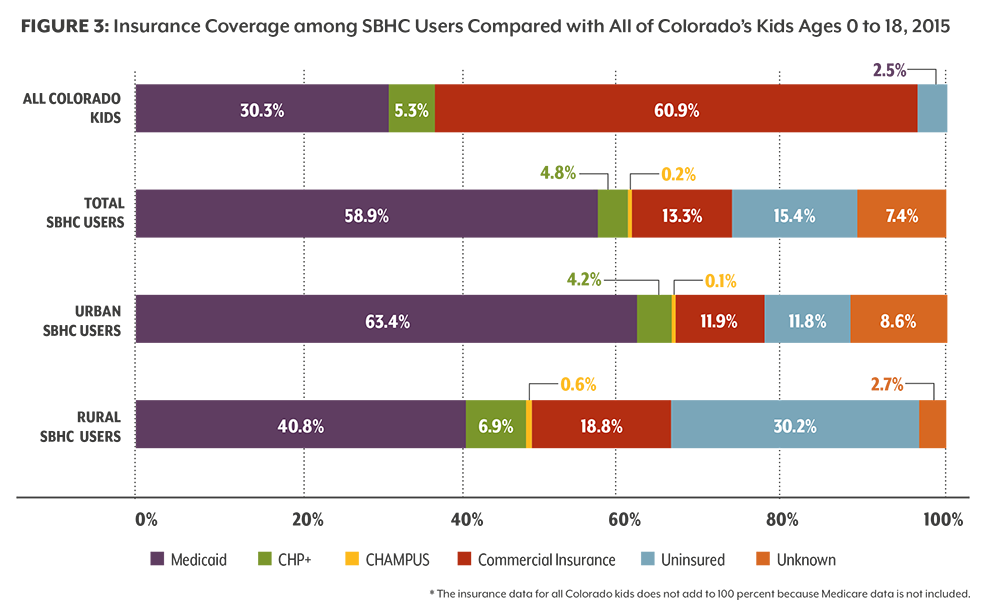
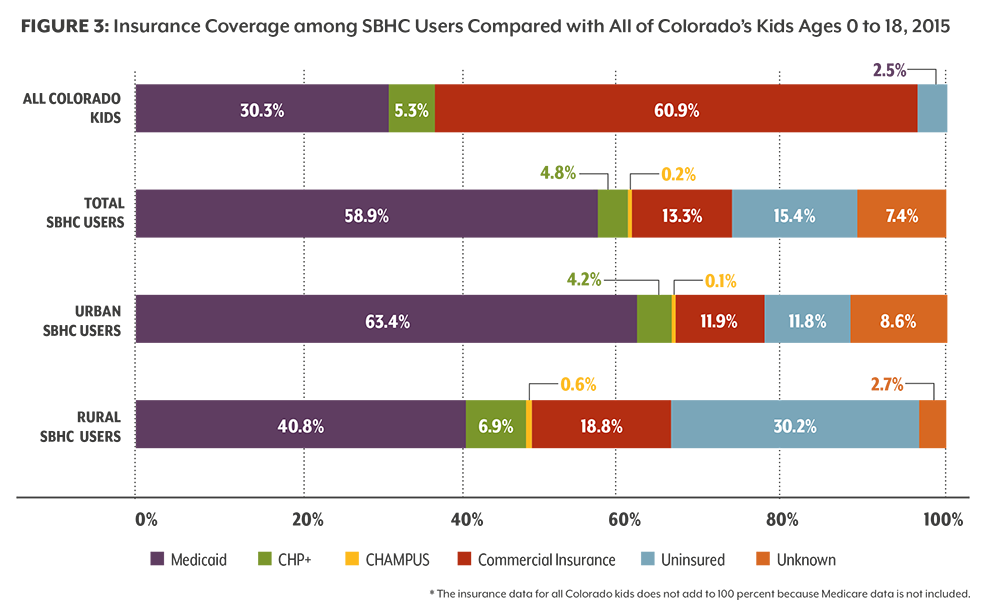
Statewide, only 2.5 percent of children and youth are uninsured, according to the 2015 Colorado Health Access Survey. But the uninsured rate among rural SBHC users is 30.2 percent — over 12 times higher than the statewide rate for children and youth (See Figure 3). A similar trend is evident in urban SBHCs. The uninsured rate for urban SBHC users is nearly five times higher than the statewide rate — 11.8 percent compared with 2.5 percent.
Nearly 41 percent of SBHC users in rural areas are covered by Medicaid compared with 63.4 percent in urban settings. Both percentages are higher than the statewide rate for young Medicaid beneficiaries (30.3 percent), reinforcing the fact that SBHCs’ mission is to serve Colorado’s most vulnerable children and youth.
SBHC Services
School-based health centers offer comprehensive care, including to users who otherwise might not have ready access to medical and behavioral services. Many services are available on-site and some by referral. These include sports physicals, screenings (vision, hearing, scoliosis); behavioral risk assessments; prescriptions for medications; and mental health assessments.
However, oral health services aren’t as widely available:
On-site dental cleanings are offered at 88.2 percent of rural SBHCs; the remaining rural SBHCs refer users to the nearest dentist’s office. Only 31.7 percent of urban sites offer on-site cleanings, and 36.6 percent refer users.
All rural SBHCs offer the application of fluoride varnish on-site compared with just over half (56.1 percent) of urban SBHCs.
Dental sealants are offered at 82.4 percent of rural SBHCs compared with 24.4 percent of urban SBHCs.
Basic mental health services, like assessments and treatment, are available at all SBHCs across Colorado, either by referral or on-site. But there is a substantial difference between rural and urban sites in substance use treatment. This service is offered on- site at almost half (47.1 percent) of rural SBHCs, and the other sites make referrals. Twenty-two percent of urban SBHCs offer this service on-site, and half refer users to another provider.
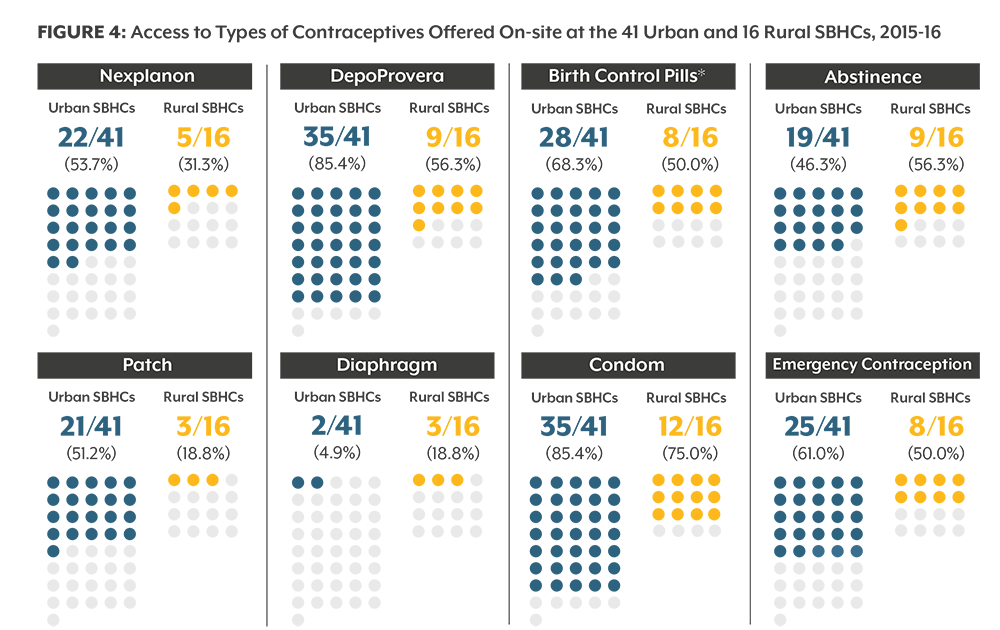
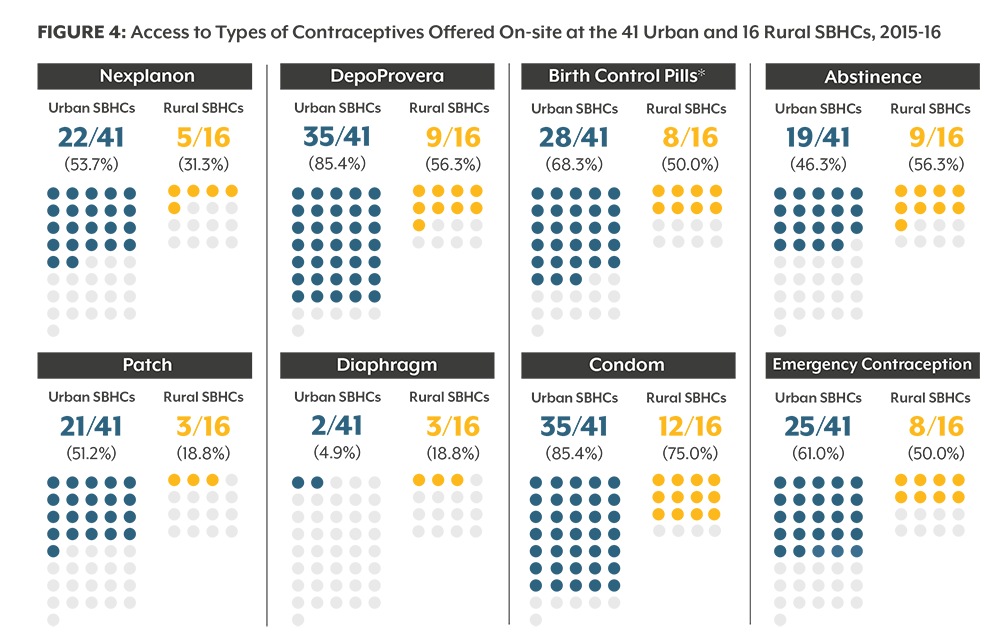
Urban SBHC users, on the other hand, have greater access to contraceptives than rural SBHCs adolescents (See Figure 4).
The biggest difference is the availability of the birth control patch. It is offered at half of urban SBHCs (51.2 percent) and about a fifth (18.8 percent) of rural sites.
Nexplanon, a birth control implant that lasts up to four years, is the most widely offered long- acting reversible contraceptive. But, again, there is a difference between urban and rural areas. Just over half of urban SBHCs (53.7 percent) offer this method compared with nearly a third of rural sites (31.3 percent).
A higher percentage of urban sites offer on-site HIV testing — 85.4 percent compared with 52.9 percent of rural SBHCs. However, the rest of the SBHCs in both settings offer this service by referral.
The availability of contraceptives at SBHCs depends on a variety of factors — school district policy, funding, provider training and skills. Access to contraceptive methods for adolescents served through SBHCs is on the rise. More clinics reported offering more methods in the 2015-16 school year than when the question first appeared on the survey the previous year.
SBHCs continue to serve Colorado’s most vulnerable users. Since the passage of the Affordable Care Act (ACA) and Medicaid expansion in Colorado, these SBHCs have seen fewer uninsured users and more Medicaid and privately insured users. Rural SBHCs, especially communities where doctors’ offices can be hard to come by.
But the future of federal health policy is unknown. Efforts by the Trump administration and Congress to repeal and replace the ACA, trim Medicaid, and give states more flexibility in health care policy could impact school- based health centers. Child Health Plan Plus (CHP+), which covers almost five percent of SBHC users across Colorado, is funded through September 2017. But it is unclear whether the federal government will continue its support past then.
Despite this uncertainty, SBHCs will remain an important provider of health care to students and others throughout the cities, plains and mountains of Colorado.
Funding Sources
Colorado’s SBHCs rely on a variety of funding streams. They include:
Federal money: Primarily from Section 330 of the Public Health Service Act, which provides grants and other financial benefits to Federally Qualified Health Centers (FQHCs), or from Health Resources and Services Administration grants that go directly to SBHCs for specific improvements.
State money: Grants are available through CDPHE to establish and maintain SBHCs across Colorado. CDPHE will receive $5 million in the 2017-18 fiscal year, the bulk of which goes to SBHCs. State money may also come from other departments, such as the Office of Behavioral Health housed within the Department of Human Services.
Local money: This may include allocations from county commissioners or grants from a school district.
Private grants and donations: Private support from foundations such as the Colorado Health Foundation and Caring for Colorado Foundation.
User revenue: Medicaid reimbursements, cash from self-pay users, etc.

{kind=link}
{kind=link}
{kind=link}
{kind=link}